Pulmonary Tuberculosis on Chest X-ray: Classic Cavitary Lesions and Volume Loss
Published on June 23, 2025

Clinical Context
A 35-year-old male presents with a 3-month history of chronic productive cough, weight loss, low-grade evening fevers, and recent hemoptysis. He reports exposure to a family member treated for tuberculosis.
Interpretation Steps
| Feature | Accuracy | Comment |
|---|---|---|
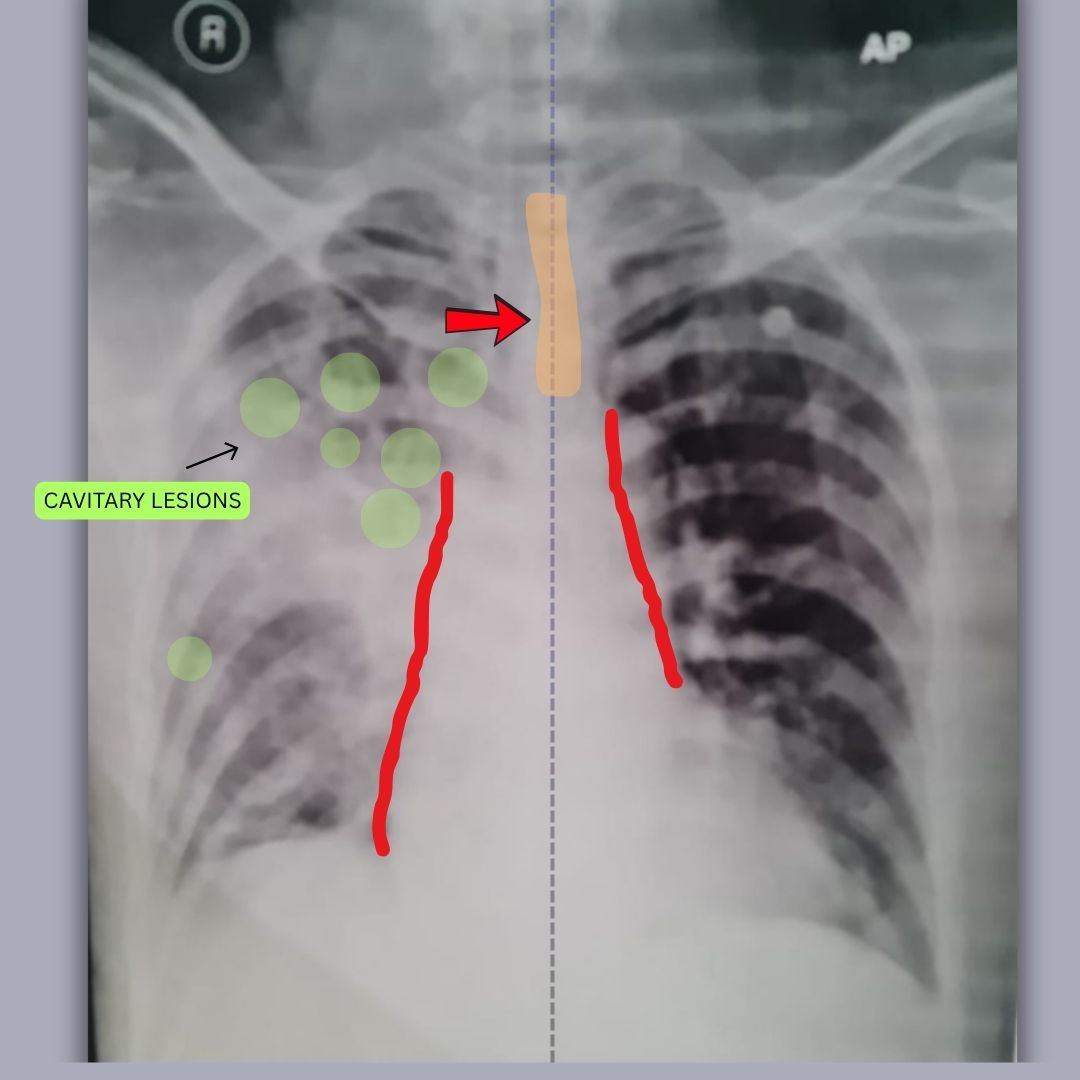
| Tracheal shift (blue arrow) | ✅ Correct | Trachea is deviated to the left—suggests left-sided volume loss. |
| Mediastinal shift (red arrow) | ✅ Correct | Pulled toward the left—classic for fibrotic lung retraction. |
| Cavitary lesions (green circles) | ✅ Correct | Well-located in the left upper/mid zones; matches TB pattern. |
| Lung field outlines (red lines) | ✅ Correct | Effectively highlights left lung volume loss and asymmetry. |
1. 🖼️ Image Quality
This is an AP (Anteroposterior) chest X-ray, indicated by the ‘AP’ label and ‘R’ marker. The image is adequately inspired and moderately well-penetrated. There’s slight rotation but acceptable for general interpretation.
2. 🌬️ Airway & Mediastinum
The trachea is visibly deviated to the left. The mediastinum, including the cardiac silhouette and central vascular structures, is also pulled toward the left. This shift strongly suggests significant volume loss in the left lung, likely the upper lobe.
3. 🫁 Breathing (Lung Fields)
-
Left Lung: The left upper and mid zones show multiple cavitary lesions. There is associated volume loss, as evidenced by mediastinal pull and tracheal deviation. This pattern is classic for post-primary (reactivation) tuberculosis. The lower zone appears relatively spared.
-
Right Lung: Hyperinflation or compensatory overaeration is noted. No overt infiltrates or cavitation seen. Lung markings are preserved.
Overall, the findings suggest chronic, likely tuberculous cavitary disease in the left upper lobe with associated fibrosis and volume loss.
4. ❤️ Circulation (Cardiac Silhouette)
The cardiac silhouette is shifted slightly to the left, in line with the mediastinal pull. The heart size appears within normal limits.
5. 📐 Diaphragm & Costophrenic Angles
The left hemidiaphragm is slightly elevated, consistent with volume loss and fibrotic retraction. Both costophrenic angles appear clear, with no visible pleural effusion.
6. 🦴 Bones & Extras
No acute bony abnormalities are identified. The clavicles and ribs are intact. No foreign objects, devices, or medical lines are seen.
✅ X-ray Findings
Left upper lobe cavitary lesions with associated volume loss, mediastinal and tracheal deviation to the left, and compensatory hyperinflation of the right lung. No effusion or acute bony abnormality noted.
Final Diagnosis
Left Upper Lobe Fibrocavitary Disease with Volume Loss, highly suggestive of Reactivation Pulmonary Tuberculosis.
Teaching Pearls
- 💡 Reactivation TB: Most commonly involves the apical and posterior segments of the upper lobes. Cavitation and fibrosis are hallmark features.
- 🫁 Cavitary Lesions: Air-filled cavities in the upper lobes raise high suspicion for TB but can also occur in fungal infections, necrotizing pneumonia, or malignancies.
- 📏 Volume Loss Indicators: Tracheal and mediastinal deviation towards the side of involvement (left here), elevated diaphragm, and rib crowding are all signs of fibrotic retraction.
Frequently Asked Questions
Q: What does upper lobe cavitation usually indicate?
A: Cavitation in the upper lobes is highly suggestive of reactivation tuberculosis but may also result from abscesses, fungal infections (e.g., aspergillosis), or necrotic malignancy.
Q: Can a chest X-ray alone diagnose TB?
A: No. While highly suggestive, especially with classic radiographic features, diagnosis requires microbiological confirmation via sputum AFB smear, culture, or molecular testing like GeneXpert.
Q: Why does the mediastinum shift toward the left here?
A: The shift is due to volume loss in the left lung, likely from fibrosis, causing traction and pulling of adjacent structures toward the affected side.