Bilateral Infiltrates & Effusions: Understanding Pulmonary Edema on X-ray
Published on June 18, 2025

Clinical Context
A 58-year-old male presents to the emergency department with acute onset of severe shortness of breath, worse when lying flat, and a productive cough with frothy sputum. He has a known history of chronic heart failure and hypertension. On examination, he is hypoxic, tachypneic, and bilateral fine crackles are audible at the lung bases.
Interpretation Steps
1. 🖼️ Image Quality
This is an AP (Anteroposterior) view of the chest, indicated by the ‘R’ marker on the right side. The image appears somewhat underexposed, making detailed assessment of subtle lung markings challenging. Inspiration appears adequate.
2. 🌬️ Airway & Mediastinum
The trachea appears central and patent. The mediastinal silhouette is within normal limits, and the cardiac contours are not overtly enlarged or displaced in this AP projection.
3. 🫁 Breathing (Lung Fields)
There are diffuse, bilateral, ill-defined patchy opacities predominantly affecting the lower and perihilar lung zones. These opacities have a somewhat fluffy, alveolar appearance. The left upper lobe appears relatively less involved, while the right mid and upper zones show some patchy haziness. Overall, the lung fields exhibit a generalized haziness, especially at the bases.
4. ❤️ Circulation (Cardiac Silhouette)
The cardiac silhouette appears to be within normal limits for size in this AP view, without clear evidence of cardiomegaly or specific chamber enlargement. Its position is central.
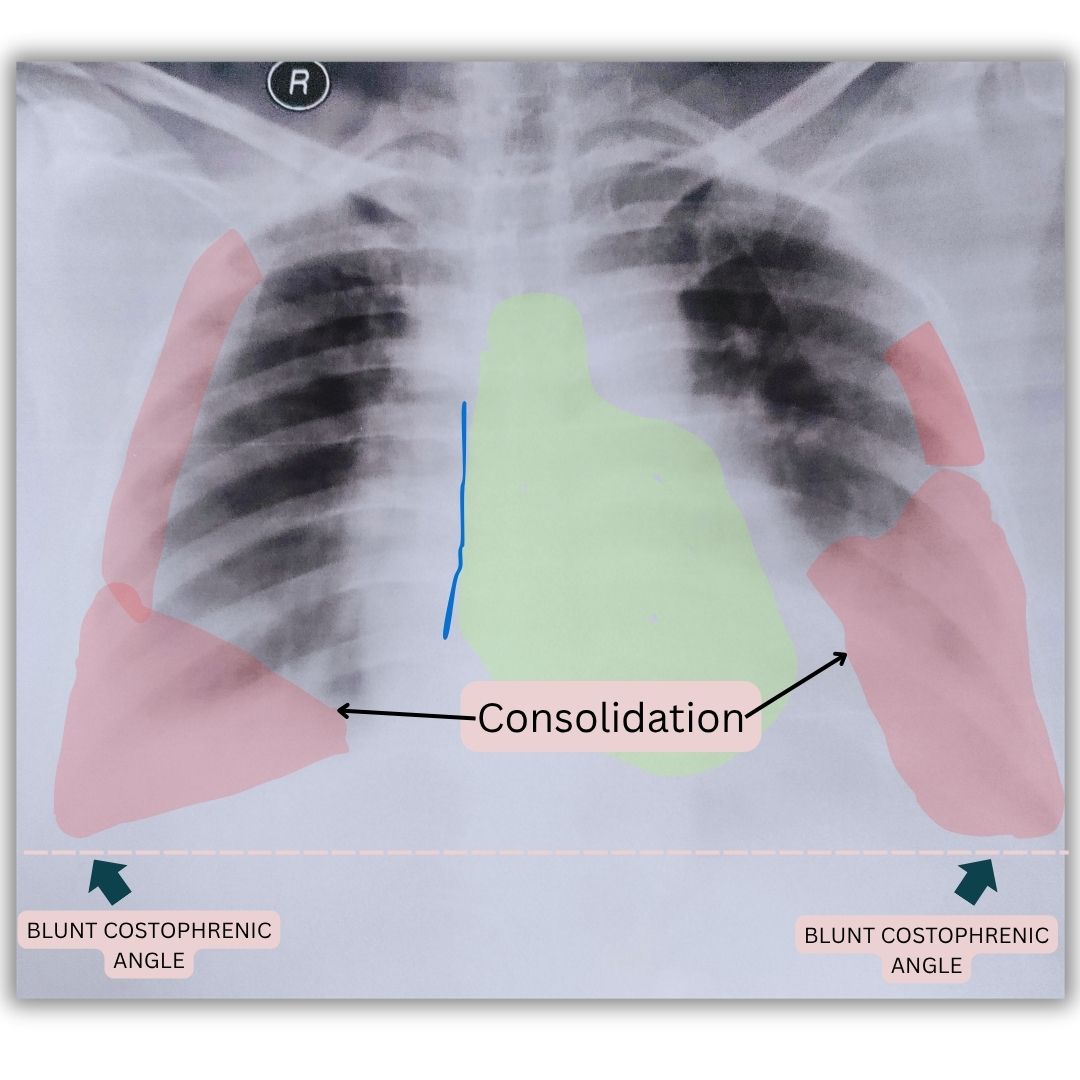
5. 📐 Diaphragm & Costophrenic Angles
Both hemidiaphragms are partially obscured by the overlying basal opacities and effusions. Both costophrenic angles are blunted, consistent with the presence of small to moderate bilateral pleural effusions.
6. 🦴 Bones & Extras
The visualized bony thorax appears unremarkable, with no obvious acute fractures or deformities. No tubes, lines, or devices are seen.
✅ X-ray Findings
Diffuse, bilateral, lower zone and perihilar patchy alveolar infiltrates. Bilateral blunting of costophrenic angles suggestive of small to moderate pleural effusions.
Final Diagnosis
Bilateral Diffuse Pulmonary Infiltrates with Pleural Effusions.
Teaching Pearls
- - 💡 Diffuse Alveolar Infiltrates: A pattern of widespread patchy or confluent opacities indicates fluid in the alveolar spaces. The differential diagnosis is broad and includes pulmonary edema (cardiogenic or non-cardiogenic ARDS), diffuse alveolar hemorrhage, widespread pneumonia (viral, atypical, or severe bacterial), and acute interstitial lung disease.
- - 💦 Bilateral Pleural Effusions: Accompanying bilateral infiltrates, effusions can point towards systemic causes like congestive heart failure, renal failure, or liver cirrhosis, or severe localized processes like widespread infection.
- - 📈 Clinical Correlation is Key: Radiographic findings of diffuse infiltrates are non-specific. The patient's clinical history (e.g., cardiac disease, renal failure, infection symptoms, acute vs. chronic onset) is paramount in narrowing the differential diagnosis and guiding further investigation and treatment.
Frequently Asked Questions
Q: What are the most common causes of bilateral diffuse pulmonary infiltrates on chest X-ray in an adult?
A: Common causes include cardiogenic pulmonary edema (congestive heart failure), Acute Respiratory Distress Syndrome (ARDS) from various etiologies (e.g., sepsis, severe pneumonia), severe bilateral pneumonia (viral, atypical, or bacterial bronchopneumonia), diffuse alveolar hemorrhage, and acute exacerbations of interstitial lung diseases.
Q: How does the presence of pleural effusions help narrow the differential diagnosis in this case?
A: Bilateral pleural effusions, especially when associated with diffuse infiltrates, strongly suggest a transudative process like congestive heart failure or fluid overload. However, they can also be seen in exudative conditions like widespread pneumonia or malignancy, so they must be interpreted in the full clinical context.
Q: What immediate investigations would be helpful to determine the cause of these findings?
A: Immediate investigations might include cardiac markers and an echocardiogram (if cardiogenic cause is suspected), blood tests (CBC, inflammatory markers, renal function, liver function), arterial blood gas, and potentially sputum or blood cultures if infection is suspected. Depending on the clinical picture, a CT scan of the chest could provide more detailed anatomical information.