Right-sided Lobar Pneumonia with Leftward Mediastinal Shift
Published on June 18, 2025
Clinical Context
A 68-year-old male presents to the emergency department with a 3-day history of high-grade fever, productive cough with yellowish sputum, and progressive shortness of breath. On examination, he is tachypneic and has dullness to percussion and bronchial breath sounds over the right lung fields.
Interpretation Steps
1. 🖼️ Image Quality
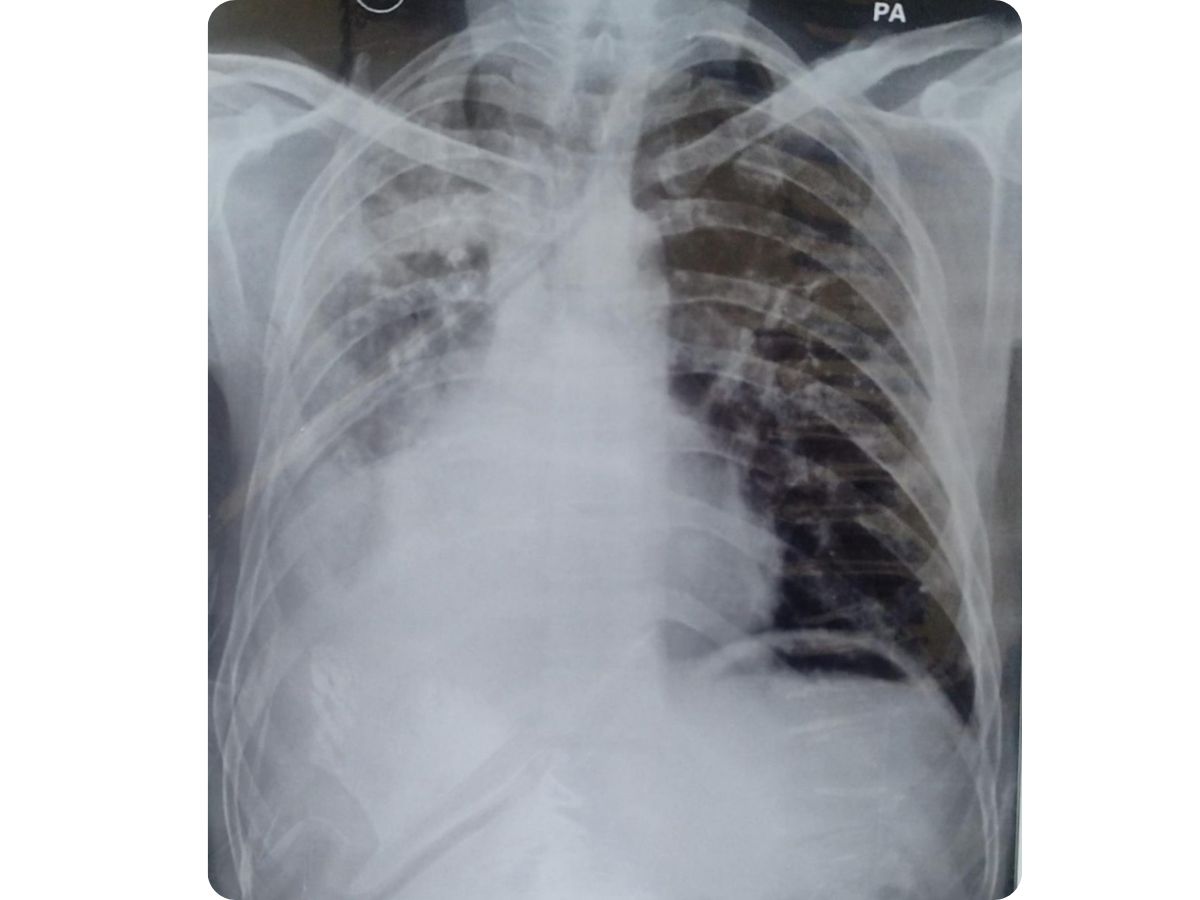
This is a PA (Posteroanterior) chest X-ray. The image demonstrates adequate inspiration and penetration. No significant rotation is noted, allowing for reliable interpretation.
2. 🌬️ Airway & Mediastinum
The trachea is notably shifted towards the left. The entire mediastinal silhouette, including the heart, is displaced significantly to the left side. This indicates a strong “pushing” effect from the right hemithorax.
3. 🫁 Breathing (Lung Fields)
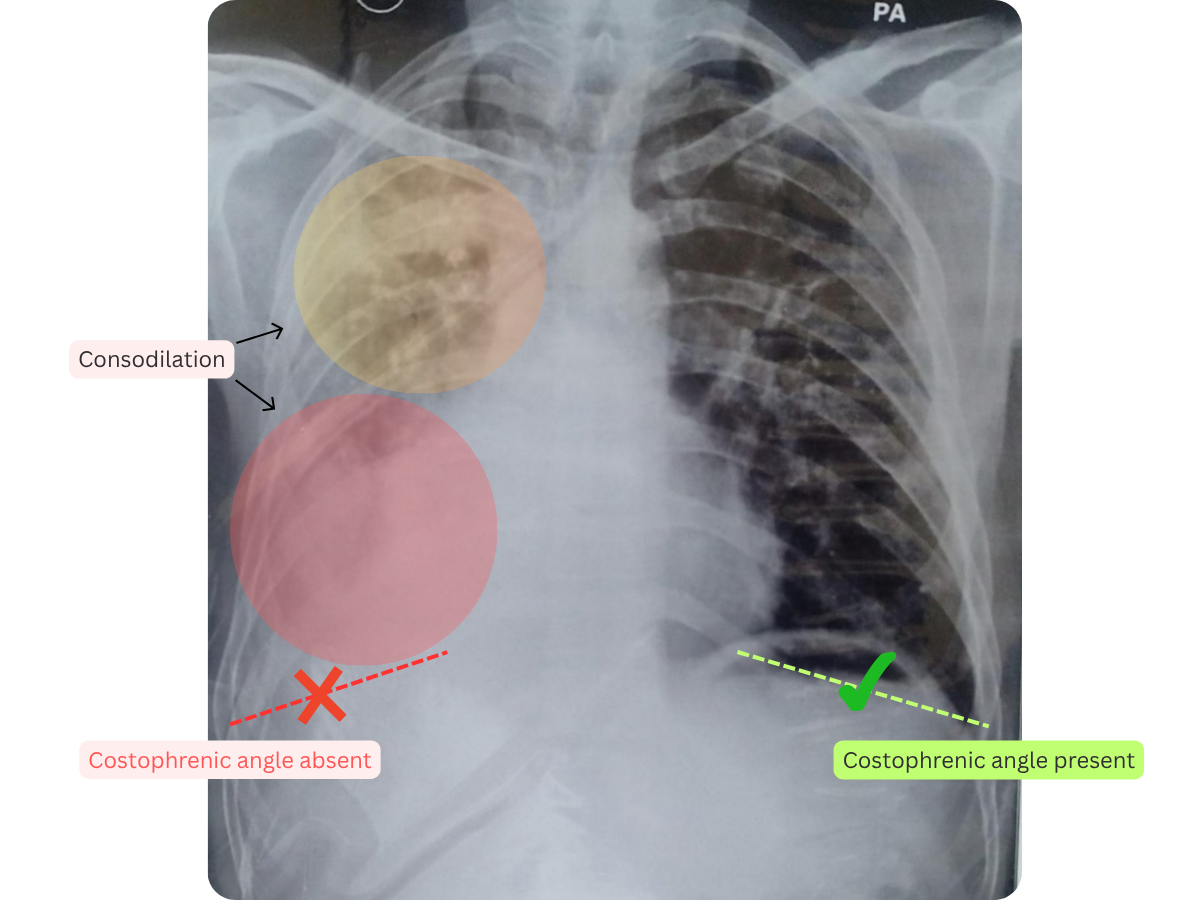
A massive, dense, and largely homogeneous opacity occupies the majority of the right hemithorax, particularly the lower and mid lung zones. This opacity completely obliterates the visualization of the right hemidiaphragm and the right heart border. There are also less dense, patchy infiltrates or reticular opacities extending into the right upper lobe. The left lung field appears relatively clear of such dense opacities, but its overall volume may appear increased due to the mediastinal shift.
4. ❤️ Circulation (Cardiac Silhouette)
The cardiac silhouette is markedly displaced to the left due to the significant volume/pressure on the right side. Its true size and specific contours are difficult to assess accurately due to this displacement and obscuration by the right-sided pathology.
5. 📐 Diaphragm & Costophrenic Angles
The right hemidiaphragm is completely obscured by the extensive right-sided opacity, and the right costophrenic angle is entirely blunted. The left hemidiaphragm and costophrenic angle appear sharp and clear.
6. 🦴 Bones & Extras
The bony thoracic cage (ribs, clavicles) appears grossly intact with no obvious acute fractures or destructive lesions. No medical devices or foreign bodies are noted.
✅ X-ray Findings
A large, dense, and homogeneous opacity is present in the right hemithorax, particularly involving the lower and mid zones, obscuring the right hemidiaphragm and heart border. Patchy infiltrates are also noted in the right upper lobe. There is a significant mediastinal shift to the left. The left lung appears relatively clear.
Final Diagnosis
Right-sided Lobar Pneumonia with Leftward Mediastinal Shift.
Teaching Pearls
- - 💡 Mediastinal Shift: A shift of the mediastinum away from the side of the pathology (as seen here to the left) is a critical sign indicating a "pushing" phenomenon. This is caused by increased volume or pressure on the affected side, such as a large consolidation, massive pleural effusion, or tension pneumothorax.
- - 🫁 Homogeneous Opacities: Large, homogeneous opacities that obscure the diaphragm and heart border are characteristic of significant consolidation (like severe pneumonia) or large pleural effusions. Clinical context and further imaging are key for differentiation.
- - 🔄 Lobar Pattern: When an inflammatory process fills the alveoli of an entire lung lobe (or multiple lobes, as suggested here), it leads to a dense, homogeneous opacity, a classic presentation of lobar pneumonia.
Frequently Asked Questions
Q: How can I definitively differentiate a large consolidation from a pleural effusion on this X-ray?
A: While both can cause similar large opacities and mediastinal shift, definitive differentiation often requires additional imaging. A CT scan of the chest would clearly distinguish between consolidated lung tissue and pleural fluid. An ultrasound can also be used to confirm the presence and nature of pleural fluid.
Q: What is the clinical significance of the mediastinal shift in this specific case?
A: The mediastinal shift signifies a large volume of pathology on the right side that is exerting pressure. While not indicating a tension pneumothorax here, it suggests a severe process (like a very large pneumonia or effusion) that can compromise cardiorespiratory function. It warrants urgent clinical assessment and management.
Q: What are the immediate next steps for a patient presenting with these X-ray findings?
A: Immediate steps include urgent clinical evaluation (assessment of respiratory distress, vital signs, oxygen saturation), laboratory tests (complete blood count, inflammatory markers, blood cultures), and prompt initiation of broad-spectrum antibiotics for suspected severe pneumonia. A CT chest scan would be crucial for precise characterization and to guide further interventions.